Discover how BIKTARVY® may benefit your patients
Prescribe with confidence
In ART naïve 1489 and 1490 studies, ≥97% efficacy (M=E analysis) after Week 48 through Week 2402
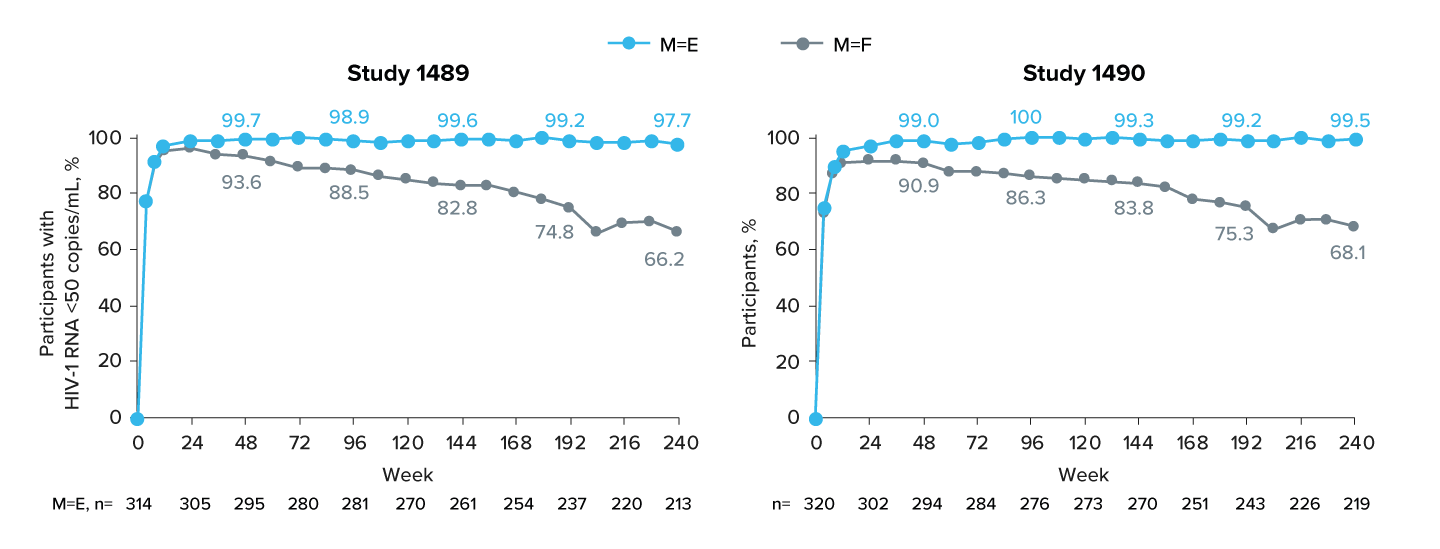
Adapted from Sax P, et al. eClinicalMedicine 2023;59:101991.
Study populations included ART-naïve people with HIV with HIV-1 RNA ≥ 500 c/mL. For further details on the study designs for the 1489 and 1490 studies click here
Among those with baseline CD4 <200 cells/μL from the pooled studies, 98% (49/50) had HIV-1 RNA <50 copies/mL at Week 240. Efficacy defined as viral load <50 copies/mL and was calculated using US FDA Snapshot algorithm; includes only participants initially randomised to BIKTARVY®.
Median CD4 changes from B/F/TAF start to Week 240, cells/μL (IQR): Study 1489: +313 (179, 475); Study 1490: +331 (215, 467)19,20
Zero treatment emergent resistance through 5 years of follow up in the ART naïve 1489/1490 studies in any group of the final resistance analysis population††2
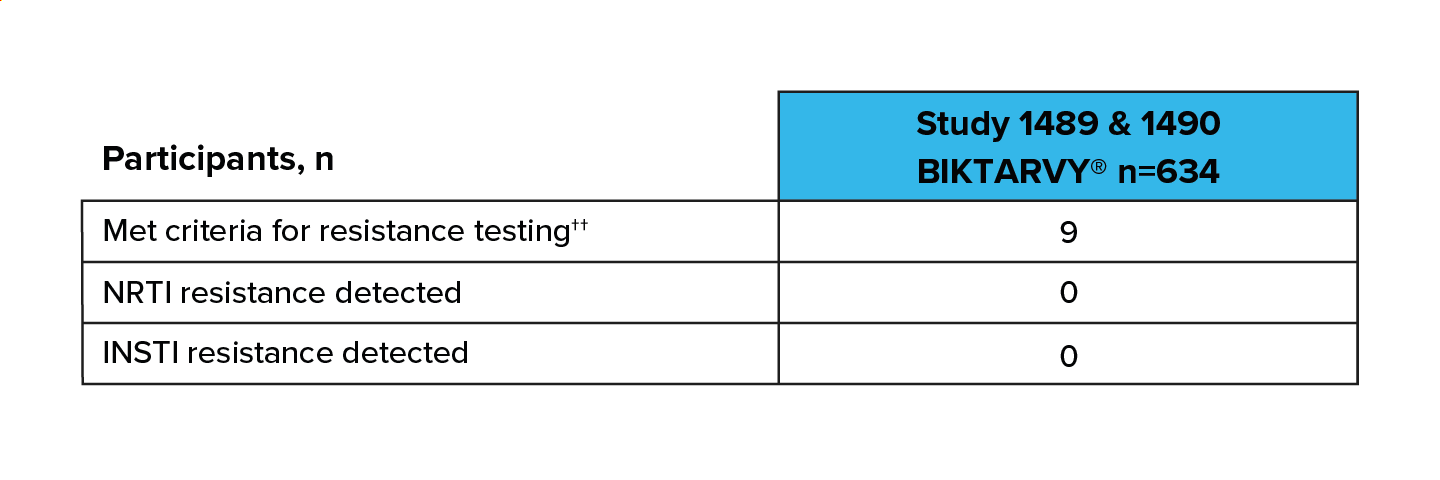
Adapted from Sax P, et al. eClinicalMedicine 2023;59:101991.
††Final resistance analysis population included participants with confirmed HIV-1 RNA ≥200 copies/mL or ≥200 copies/mL at last visit, with no resuppression of HIV-1 RNA to <50 copies/mL while on study drug; includes only participants initially randomised to BIKTARVY®.2
You might also like


Focus on long-term health
Understand how BIKTARVY® could impact your patient's quality of life
Footnotes:
*Robust: Defined as maintained efficacy, which is dependent on patient adherence. Adherence is impacted by tolerability and simplicity of treatment.21–24
§Efficacy: In RCTs in treatment-naïve participants, BIKTARVY® was non-inferior (VL <50 copies/mL) to ABC/3TC/DTG (Study 1489) and DTG + FTC/TAF (Study 1490) at Weeks 48 (primary endpoint), 96 and 144 (secondary endpoints).1 Pooled efficacy for BIKTARVY® (VL <50 copies/mL, n=634, M=F) at Weeks 48 and 144 was 91% and 82% respectively.1 After the optional 96 week open-label extension phase (from Weeks 144 through 240), participants taking BIKTARVY® since baseline achieved and maintained high rates of virologic suppression (VL <50 copies/mL: 99% [n=426/432] M=E, 67% [n=426/634] M=F).2 In RCTs in virologically suppressed participants, BIKTARVY® was non-inferior (VL≥50 copies/mL, M=F) at the Week 48 primary endpoint to comparator regimens of ABC/3TC/DTG (Study 1844) and ATV- or DRV-based regimens (Study 1878).1 BIKTARVY® efficacy at Week 48 (VL <50 copies/mL, M=F) was 94% in Study 1844 (n=282) and 92% in Study 1878 (n=290).1 Participants who switched to BIKTARVY® at baseline or from Week 48 in an optional open-label extension (Study 1844 total exposed to BIKTARVY® n=547, Study 1878 n=534) maintained high levels of viral suppression (VL <50 copies/mL, M=E) through 96 weeks in Study 1844 (100%, n=283/283)3 and Study 1878 (100%, n=318/318).4
ΩPivotal: defined as the four registrational trials for BIKTARVY® (Studies 1489, 1490, 1844 and 1878).
Resistance: In pivotal (registrational) Phase 3 RCTs, there was 0 treatment-emergent resistance to the components of BIKTARVY® in the final resistance analysis populations.1–5
Abbreviations:
3TC, lamivudine; ABC, abacavir; ART, antiretroviral therapy; ATV, atazanavir; CD4, cluster of differentiation 4; DRV, darunavir; DTG, dolutegravir; eGFRCG; estimated glomerular filtration rate (Cockcroft-Gault); HBV, hepatitis B virus; HCV, hepatitis C virus; HIV, human immunodeficiency virus; INSTI, integrase strand transfer inhibitor; IQR, interquartile range; M=E, missing=excluded; M=F, missing=failure; NRTI, nucleoside reverse transcriptase inhibitor; PRT, proximal renal tubulopathy; RNA, ribonucleic acid; SmPC, Summary of Product Characteristics; VL, viral load.
References:
- BIKTARVY® Summary of Product Characteristics.
- Sax P, et al. eClinicalMedicine 2023;59:101991.
- Brar I, et al. Infectious Diseases (ID) Week 2020, 21–25 October. Poster 1028.
- Rockstroh JK, et al. HIV Glasgow 2020, 5–8 October; Glasgow, UK. Poster 036.
- Orkin C, et al. HIV Glasgow 2022, 23–28 October; Glasgow, UK. Poster P088.
- Gallant J, et al. Lancet 2017;390:2063–2072.
- Sax PE, et al. Lancet 2017;390:2073–2082.
- Kityo C, et al. International AIDS Society (IAS) 2019, 21–24 July; Mexico City, Mexico. Presentation MOAB0106.
- Molina JM, et al. Lancet HIV 2018;5:e357–e365.
- Daar ES, et al. Lancet HIV 2018;5:e347–e356.
- Podzamczer D, et al. HIV Glasgow 2018, 28–31 October: Glasgow, UK. Poster 119.
- Mills A, et al. Conference on Retroviruses and Opportunistic Infections (CROI) 2020, 8–11 March: Boston MA. Poster 2886.
- Maggiolo F, et al. HIV Med 2023;24:27−36.
- Hagins D, et al. J Acquir Immune Defic Syndr 2021;88:86−95.
- Natukunda E, et al. 13th International Workshop on HIV Pediatrics 2021. Virtual meeting. Available at: https://www.natap.org/2021/IAS/IAS_80.htm. Accessed February 2026.
- Trottier B, et al. HIV Glasgow 2022, 23–26 October 2022; Glasgow, UK. Poster P067.
- Gilead. Data on file HIV116. March 2022.
- Post F, et al. Conference on Retroviruses and Opportunistic Infections (CROI) 2025, 9–13 March; San Francisco, United States. Poster 859.
- Workowski K, et al. Conference on Retroviruses and Opportunistic Infections (CROI) 2021, 6–10 March. Abstract 415.
- Wohl D, et al. Conference on Retroviruses and Opportunistic Infections (CROI) 2022, 12–24 February: virtual. Abstract 494.
- US Department of Health and Human Services (DHHS). What to Start: Guidelines for the Use of Antiretroviral Agents in Adults and Adolescents Living with HIV, March 2023. Available at: https://clinicalinfo.hiv.gov/sites/default/files/guidelines/documents/adult-adolescentarv/guidelines-adult-adolescent-arv.pdf. Accessed February 2026.
- Cihlar T, et al. Curr Opin Virol 2016;18:50–56.
- Trottier B, et al. J Int AIDS Soc 2014;17(Suppl 3):19765.
- Orkin C, et al. HIV Med 2018;19:18–32.
UK-BVY-0703 Date of preparation February 2026