Focus on long-term health
BIKTARVY® had significantly fewer all-grade treatment-related AEs vs DTG plus ABC/3TC or FTC/TAF (secondary endpoint) with low and similar rates of discontinuation across all arms6,8,9
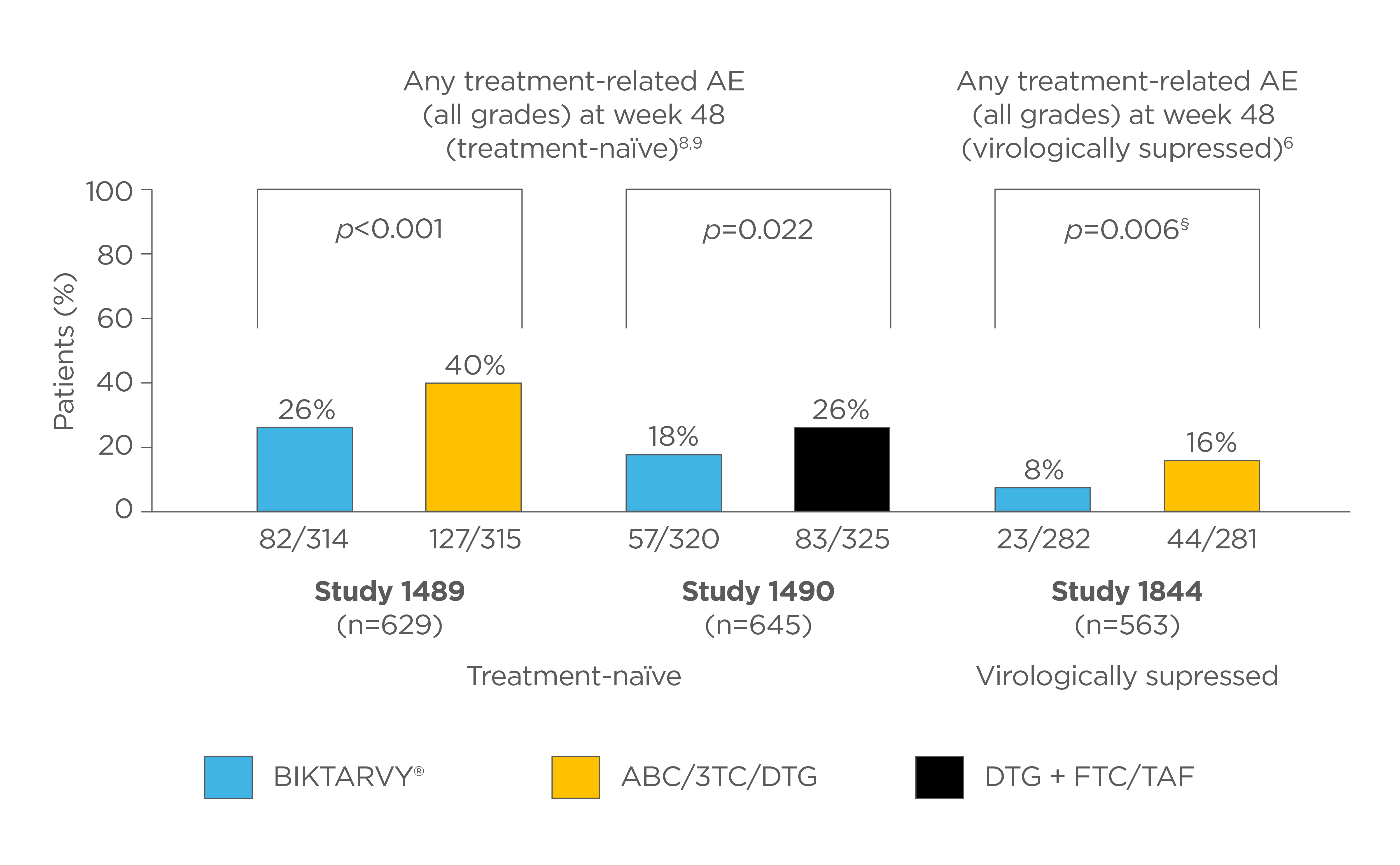
Adapted from: Molina JM, et al. Lancet HIV 2018;5:e357–e365, Gallant J, et al. Lancet 2017;390:2063–2072 and Sax PE, et al. Lancet 2017;390:2073–2082.
§Fisher’s exact test.6
Comparisons between trials cannot be made as head-to-head comparison.
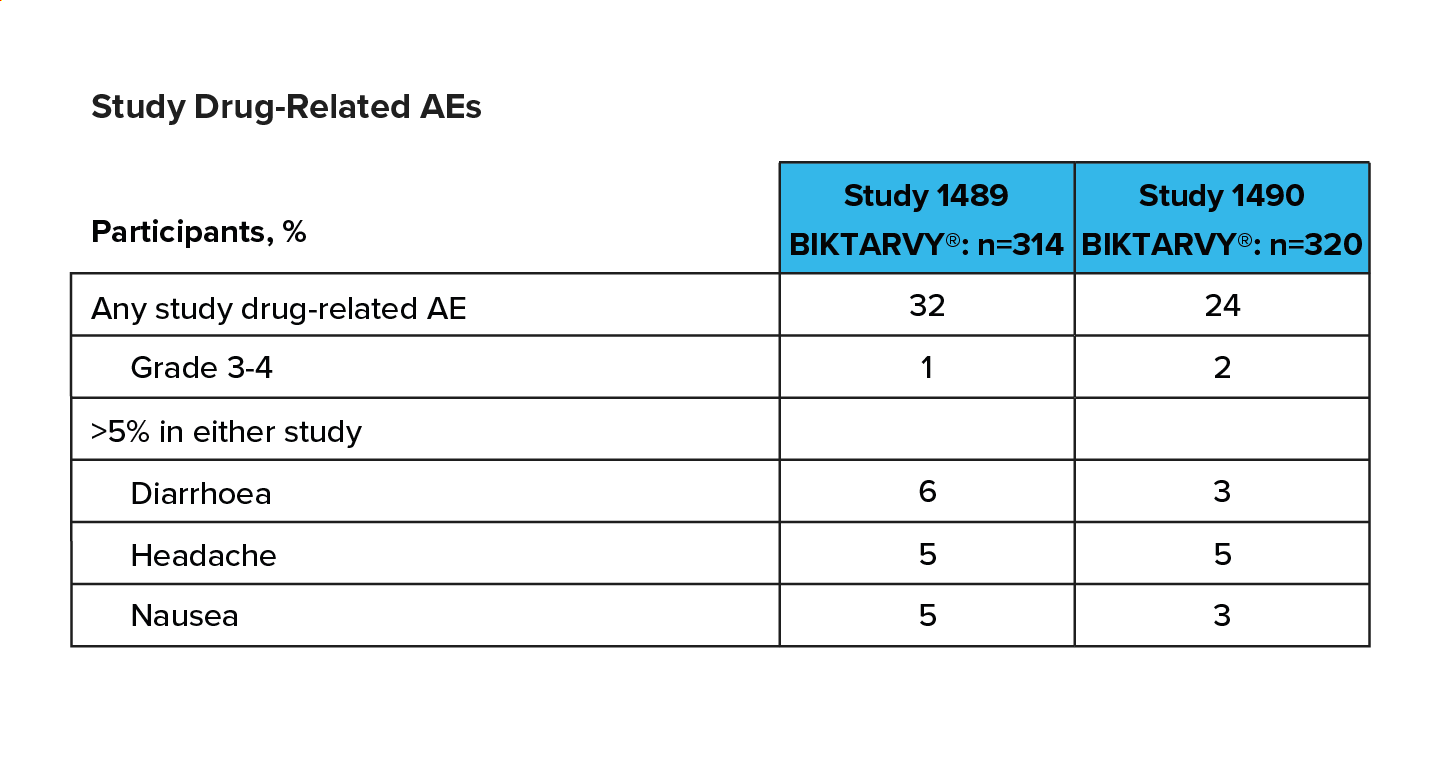
Through to Week 240, grade 3-4 treatment-related AEs occurred in 2% of participants taking BIKTARVY® in the ART naïve studies 1489 and 149010
Adapted from: Wohl D, et al. Conference on Retroviruses and Opportunistic Infection (CROI) 2022, 12–24 February; Virtual. Abstract 494.
AEs were mostly Grade 1 and rarely led to discontinuation, Over the 5 years, 10 of the 634 participants (pooled Study 1489 and Study 1490 data) discontinued BIKTARVY® due to an adverse event, of which only 4 were considered related to BIKTARVY® by the investigator.10
PROs in ART naïve and switch populations with BIKTARVY® vs ABC/3TC/DTG - Studies 1489 and 184411
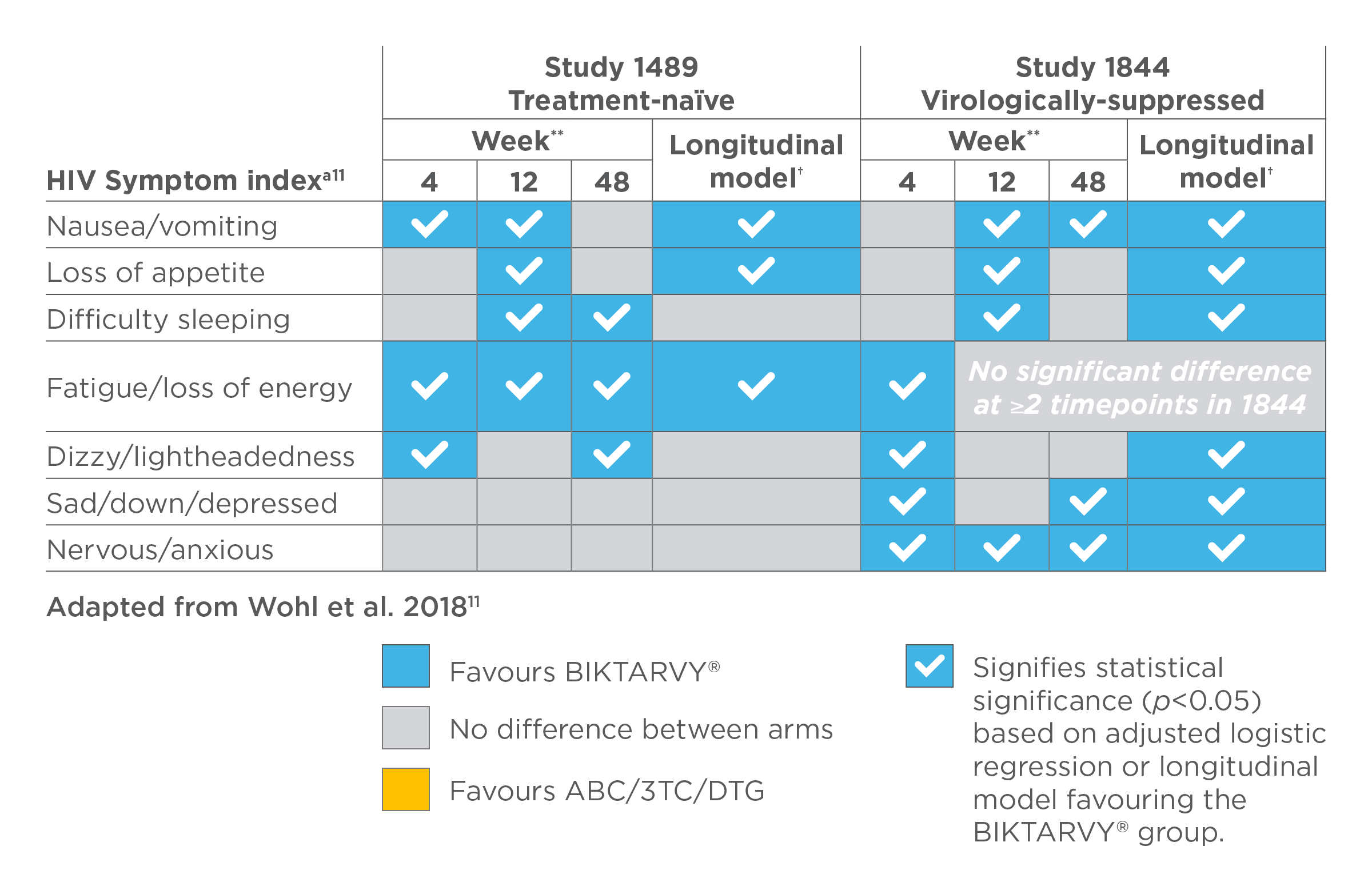
aOnly symptoms where ≥2 time points/models showed significance in either study are presented; The HIV symptoms distress module (HIV-SI) was administered at baseline and weeks 4, 12, and 48. Responses to each of the 20 items were dichotomised as bothersome or not bothersome. For 15/20 (in Study 1489) and 14/20 (in Study 1844) items, there was no difference in prevalence observed between groups from week 4 to week 48; TICK = Statistically significant (p<0.05), based on the adjusted logistic regression model, favouring the B/F/TAF group over the ABC/3TC/DTG group.
**Multivariate regression model controlled for age, sex, race, baseline HIV Symptom Index score, VACS Index, history of serious mental illness, baseline SF-36 physical and mental scores, and years since diagnosis (for study 1844 only).
†Longitudinal modelling was performed using generalised mixed-effects models to show symptom patterns over each of the four study visits.
PROs showed greater sleep quality with BIKTARVY® vs ABC/3TC/DTG in virologically suppressed people living with HIV (Study 1844)11
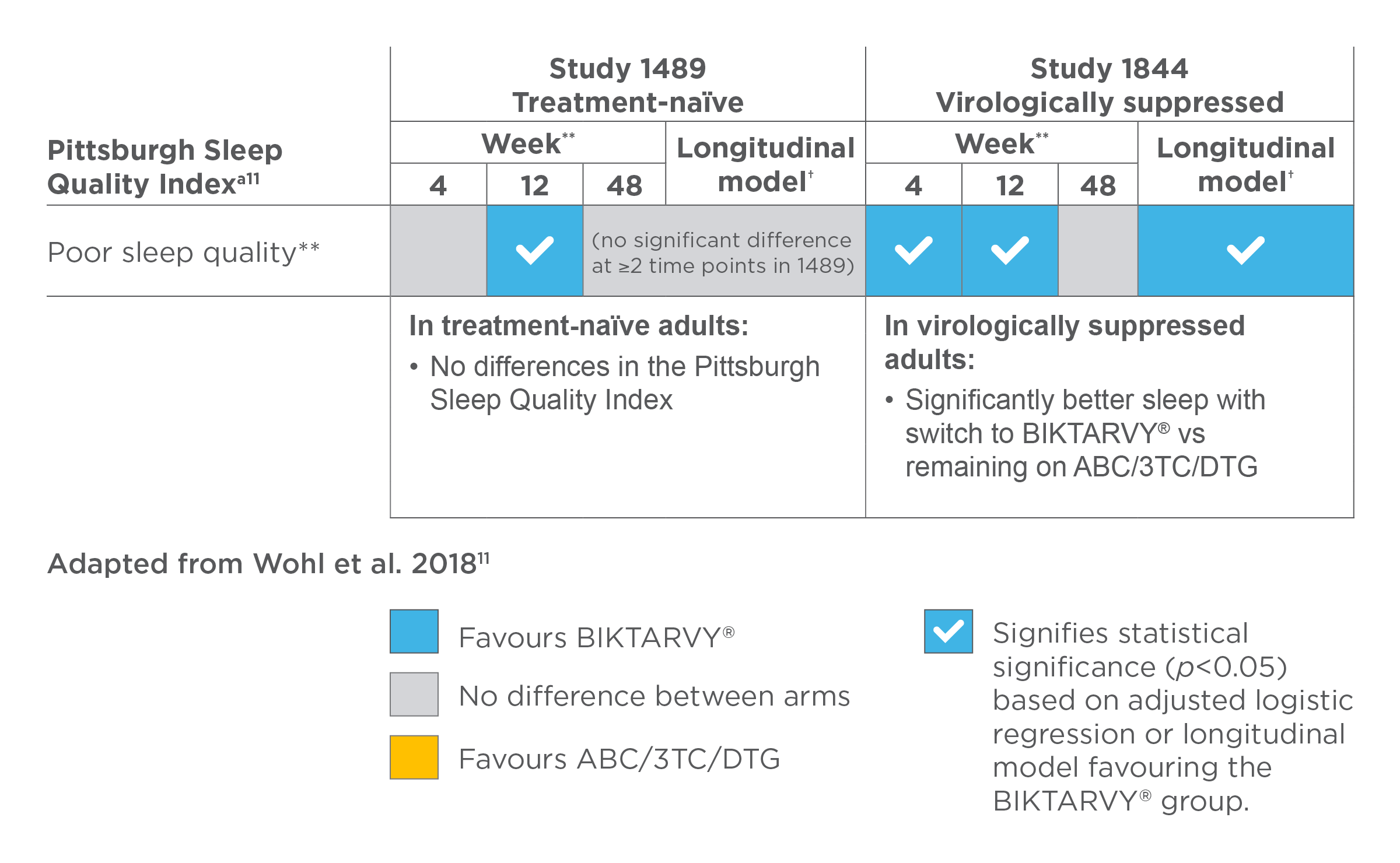
aOnly symptoms where ≥2 time points/models showed significance in either study are presented; TICK = Statistically significant (p<0.05), based on the adjusted logistic regression model, favouring the B/F/TAF group over the ABC/3TC/DTG group.
**Multivariate regression model controlled for age, sex, race, baseline HIV Symptom Index score, VACS Index, history of serious mental illness, baseline SF-36 physical and mental scores, and years since diagnosis (for study 1844 only).
†Longitudinal modelling was performed using generalised mixed-effects models to show symptom patterns over each of the four study visits.
You might also like


Footnotes:
*Pivotal: Defined as the four registrational trials for BIKTARVY® (studies 1489, 1490, 1844 and 1878).
‡Tolerability and discontinuation due to adverse events (AEs): In Studies 1489 and 1490 of treatment-naïve participants receiving BIKTARVY® through 144 weeks, the most frequently reported AEs were headache (5%), diarrhoea (5%) and nausea (4%).1 In these studies, discontinuation due to AEs was 1% at Week 48,1 1% at Week 144 (n=6/634)12 and 1.6% (n=10/634) at week 2402 for participants initially randomised to BIKTARVY®. Cumulative deaths were reported in 1,8,9 612 and 92 (1.4%) participants by weeks 48, 144 and 240.
In virologically suppressed participants at Week 48, 2% (6/282) discontinued BIKTARVY® due to AEs in Study 1844, and 1% (2/290) in Study 1878.6,7 Across both studies (1844 and 1878), <2% of the 1081 participants discontinued treatment with BIKTARVY® due to AEs through the open label extension study phase.3,4 By week 48, death was reported in 2 (1%) and 1 (<1%) of participants in studies 18446 and 18787 respectively. One participant in the 1844 study died during OLE phase.3 Please refer to the SmPC for the full list of AEs and product safety profile.
Abbreviations:
3TC, lamivudine; ABC, abacavir; AE, adverse event; DTG, dolutegravir; FTC, emtricitabine; HIV, human immunodeficiency virus; HIV-SI, HIV Symptoms Index; RNA, ribonucleic acid; SF-36, 36-item Short Form Health Survey; SmPC, Summary of Product Characteristics; TAF, tenofovir alafenamide; VACS, veterans aging cohort study.
References:
- BIKTARVY® Summary of Product Characteristics.
- Sax P, et al. eClinicalMedicine 2023;59:101991.
- Brar I, et al. Infectious Diseases (ID) Week 2020, 21–25 October. Poster 1028.
- Rockstroh JK, et al. HIV Glasgow 2020, 5–8 October; Glasgow, UK. Poster 036.
- Orkin C, et al. HIV Glasgow 2022, 23–28 October; Glasgow, UK. Poster P088.
- Molina JM, et al. Lancet HIV 2018;5:e357–e365.
- Daar ES, et al. Lancet HIV 2018;5:e347–e356.
- Gallant J, et al. Lancet 2017;390:2063–2072.
- Sax PE, et al. Lancet 2017;390:2073–2082.
- Wohl D, et al. Conference on Retroviruses and Opportunistic Infection (CROI) 2022, 12–24 February; Virtual. Abstract 494.
- Wohl DA, et al. Patient 2018;11:561–573.
- Orkin C, et al. Lancet HIV 2020;7:e389–e400.
UK-BVY-0703 Date of preparation February 2026